The tracing shown is from a woman at 28-weeks gestation in the post-anesthesia care unit (PACU) after an appendectomy. She is alert and awake. Based on this fetal heart rate pattern, the most appropriate intervention is:
Administer terbutaline
Continued monitoring
Perform cesarean birth
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
The fetal heart rate tracing shows:
Baseline around 140 bpm
Minimal variability
No accelerations
No decelerations
Regular uterine activity but not tachysystole
This pattern is Category II, but in the context of:
28-week gestation
Immediate postoperative status after anesthesia
Maternal alertness and stability
NCC and AWHONN emphasize that maternal sedation, post-anesthesia effects, medications, and physiologic stress commonly cause temporary minimal variability without acidemia, especially at preterm gestations where baseline variability is normally lower.
Key NCC principle:
Minimal variability in a stable mother without decelerations does NOT require emergent delivery.
Instead, the fetus should be observed as anesthesia effects wear off.
Why other answers are incorrect:
A. Terbutaline – No tachysystole and no recurrent decels are present.
C. Cesarean birth – No bradycardia, no late decels, no absent variability, and no Category III criteria.
Thus, appropriate management is B. Continued monitoring.
Nonstress testing is used more frequently for antepartum testing than contraction stress testing because contraction stress testing has a:
Higher frequency of equivocal test results
Limited reporting option for the compromised fetus
Low predictability of fetal well-being within 7 days of a negative test
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
NCC and AWHONN explain that Contraction Stress Testing (CST):
Has a higher rate of equivocal (“equivocal–suspicious” or “equivocal–hyperstimulation”) results
Frequently must be repeated or replaced with other tests
Requires inducing contractions, which carries risk (hyperstimulation, preterm labor, uterine rupture in scarred uterus)
NST is used more commonly because it is:
Noninvasive
Easier to perform
Has fewer contraindications
Has a lower rate of equivocal results
Why the others are incorrect:
B — CST does detect fetal compromise reliably and is NOT limited in its reporting structure.
C — A negative CST actually has very high negative predictive value for 7 days, making this answer incorrect.
Thus the correct choice is A. Higher frequency of equivocal results.
A nulliparous woman at term presents with leaking fluid. Rupture of membranes confirmed. After 6 hours she is completely dilated, +2 station, has been pushing 2 hours with oxytocin at 10 mU/min. The fetal tracing is shown. What is the next step in management?
Continue pushing for another hour
Decrease oxytocin
Expedite birth
Comprehensive and Detailed Explanation From Exact Extract Without Any URLs or Links:
According to the NCC C-EFM 2025 Exam Content Outline and recommended references such as AWHONN Fetal Heart Monitoring Principles, Simpson & Miller (Fetal Monitoring Text), and Menihan’s EFM Guide, recurrent variable or late decelerations with minimal or moderate variability during the second stage of labor—particularly when the patient has been pushing for ≥2 hours—indicate progressive fetal intolerance of labor.
AWHONN states that when the fetal tracing displays recurrent variable decelerations with ongoing stress from long second stage, the recommended intervention is operative or expedited vaginal birth, provided the fetal station is at +2 or lower. AWHONN and Simpson emphasize that reducing oxytocin is insufficient when the tracing demonstrates ongoing significant decelerations during active pushing with adequate descent.
The NCC blueprint within Pattern Recognition & Intervention emphasizes:
Identifying worsening recurrent decelerations
Acting when fetal tolerance is decreasing
Prioritizing timely intervention when the second stage exceeds standard limits with a non-reassuring tracing
Because she is fully dilated, vertex at +2, and tracing shows recurrent decelerations during pushing, the evidence-based next step is expediting birth, typically via operative vaginal delivery.
(Full question)
This tracing would be categorized as a
Category I
Category II
Category III
Comprehensive and Detailed Explanation From Exact Extract (No URLs):
According to AWHONN Fetal Heart Monitoring Principles & Practice, Simpson & Miller, and the NCC C-EFM Content Outline, fetal heart rate categories are assigned based on baseline, variability, presence/absence of accelerations, and type of decelerations.
A Category II tracing includes any pattern that is not clearly normal (Category I) or clearly abnormal (Category III). Classic Category II features include:
• Bradycardia NOT accompanied by absent variability
• Tachycardia
• Minimal variability
• Marked variability
• Absence of accelerations after stimulation
• Recurrent variable decelerations with minimal or moderate variability
• Prolonged decelerations (≥2 min but <10 min)
In this tracing, the fetus demonstrates:
– A prolonged deceleration with subsequent recovery,
– Presence of baseline variability,
– Return toward baseline but not immediately normal.
AWHONN and Simpson state that any prolonged deceleration automatically places the tracing in Category II unless variability is absent (which would escalate it to Category III). Because variability is present, it cannot be Category III.
Therefore, by NCC standards, this tracing is Category II.
The fetal heart rate tracing shown represents
category I
category II
category III
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources
The tracing demonstrates a baseline within normal limits, moderate variability, and recurrent variable decelerations associated with contractions. According to NICHD/NCC definitions reproduced in AWHONN’s Fetal Heart Monitoring Principles & Practices and Menihan’s Electronic Fetal Monitoring, recurrent variable decelerations with preserved variability classify the tracing as Category II.
A Category I pattern must show baseline 110–160, moderate variability, and absence of late or variable decelerations. Because this tracing shows recurrent variable decelerations, it does not meet Category I criteria.
Category III requires absent variability PLUS recurrent late decelerations, recurrent variable decelerations, bradycardia, or a sinusoidal pattern. This tracing shows moderate variability, therefore it cannot be Category III.
Simpson & Creehan emphasize that variable decelerations reflect cord compression and fall into Category II unless accompanied by absent variability. Miller’s Pocket Guide confirms that moderate variability maintains fetal compensatory reserve, keeping the pattern in Category II.
(Full question statement)
A woman at 39-weeks gestation is in labor, progressing normally. The baseline fetal heart rate has increased from 125 to 150 beats per minute over the last hour with moderate variability. What is the next step?
Continue to observe
Initiate antibiotic therapy
Perform an ultrasound
Comprehensive and Detailed Explanation From Exact Extract Without Links:
NCC-recommended references (Simpson, AWHONN FHM, Creasy & Resnik) note that baseline increases within the normal range (110–160 bpm) accompanied by moderate variability are typically benign. Mild physiologic causes—maternal activity, fetal stimulation, or normal sympathetic activation—may transiently raise baseline FHR.
AWHONN stresses that intervention is required only when tachycardia exceeds 160 bpm or when variability is minimal/absent or accompanied by recurrent decelerations.
Here, the baseline increase to 150 bpm remains within normal limits and is paired with moderate variability, which the NCC recognizes as the strongest indicator of adequate fetal oxygenation.
Therefore, evaluation is complete, and continued observation is the appropriate course.
A woman at 34-weeks gestation is in active labor after spontaneous rupture of membranes. Accelerations should be documented as
absent
present 10×10
present 15×15
Comprehensive and Detailed Explanation From Exact Extract (No URLs)
For fetuses before 32–34 weeks, the National Certification Corporation (NCC) follows the physiologic standards established by AWHONN, Simpson & Creehan, Menihan, and Creasy & Resnik, which emphasize that preterm fetuses have less mature autonomic nervous system development, resulting in smaller and shorter accelerations.
According to the NCC C-EFM Exam Content Outline (Pattern Recognition & Intervention) and the AWHONN Fetal Heart Monitoring Principles (2022–2024):
Preterm fetuses (<32 weeks) normally demonstrate 10 bpm × 10 sec accelerations.
By approximately 32–34 weeks, accelerations may begin transitioning toward 15×15, but the accepted standard for documentation at 34 weeks remains 10×10, unless clearly meeting 15×15 criteria.
NCC emphasizes using gestational-age–appropriate criteria for documenting accelerations, because autonomic reactivity increases gradually and is not fully comparable to term until after 32–34 weeks.
Menihan’s Electronic Fetal Monitoring also states that preterm fetuses “should be evaluated with the 10×10 rule until it is clear that the fetus is demonstrating mature 15×15 acceleratory capacity.”
Simpson & Creehan reinforce this point, noting that accelerations in late preterm gestations “may not consistently reach 15 bpm for 15 seconds, and thus 10×10 remains the appropriate designation.”
Since the patient is 34 weeks, the fetus is late-preterm and may not reliably meet the full 15×15 criteria; therefore, the correct documentation standard remains 10×10.
Thus, accelerations should be charted as:
“Present 10×10.”
References
NCC C-EFM Candidate Guide 2025 – Content Domain: Pattern Recognition and Intervention
AWHONN Fetal Heart Monitoring Principles & Practices, 2022–2024
Menihan: Electronic Fetal Monitoring: Concepts and Applications
Simpson & Creehan: Perinatal Nursing
Miller: Fetal Monitoring Pocket Guide
Creasy & Resnik: Maternal–Fetal Medicine
Upon admission, the clinician discusses indications, risks, and benefits of electronic fetal monitoring. This reflects which ethical concept?
Autonomy
Fiduciary
Informed consent
Comprehensive and Detailed Explanation From Exact Extract Without Any URLs or Links:
The NCC C-EFM Professional Issues domain identifies informed consent as a fundamental ethical requirement in fetal monitoring. AWHONN’s perinatal nursing standards state that the clinician must provide clear explanation of risks, benefits, alternatives, and the purpose of EFM, ensuring the patient makes a voluntary and informed decision.
Simpson, Creasy & Resnik, and ACOG-referenced materials used by NCC emphasize that informed consent is the process, while autonomy is the principle that supports it. The act of explaining EFM and its implications is therefore informed consent, not autonomy itself.
In the NCC competencies, clinicians must:
Provide accurate information
Support shared decision-making
Verify maternal understandingThis exactly matches the process of informed consent, not merely respecting autonomy or acting as a fiduciary.
A woman (G1P0) arrives in triage with a pain score of 4/10 at 39-weeks gestation. The fetal heart rate tracing shown is obtained. The best intervention is to:
Adjust tocotransducer and continue to monitor
Admit for induction
Discharge to home
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
This tracing demonstrates a normal, reassuring fetal heart pattern that is technically categorized as Category I, indicating normal fetal acid–base status. Before any decision regarding discharge or induction, NCC emphasizes correct assessment of the tracing quality, fetal status, and uterine activity.
Key Tracing Characteristics
Baseline:Approximately 135–145 bpm, well within the normal range of 110–160 bpm.
Variability:The strip shows moderate variability (6–25 bpm), the strongest indicator of adequate fetal oxygenation per NCC, AWHONN, and NICHD.
Accelerations:Several accelerations are present—another reassuring feature of normal fetal well-being.
Decelerations:No variable, late, or prolonged decelerations are present.
Uterine Activity:The lower channel shows poor recording quality and inconsistent signal—suggesting the toco is not capturing contractions well, not that the patient is contracting excessively or not at all.
Correct interpretation per NCC:
NCC emphasizes distinguishing between physiologic assessment and technical artifact.
The fetal tracing is completely reassuring.
The only abnormality is the poor uterine activity signal, a common triage occurrence due to:
Toco placement
Maternal body habitus
Positioning
Low contraction intensity in early labor
Thus, the correct next step is to optimize equipment (reposition the toco, adjust belt, palpate contractions) and continue to monitor.
Why the other options are incorrect:
B. Admit for induction – NOT indicated
There is no evidence of fetal compromise.
No indication for induction is present (pain score 4/10, reassuring FHR, term pregnancy).
NCC emphasizes avoiding unnecessary interventions.
C. Discharge to home – NOT yet appropriate
You cannot safely discharge a patient with a poorly monitored contraction pattern.
Adequate assessment requires confirming uterine activity—after fixing the toco.
Therefore, the appropriate action is:
A. Adjust tocotransducer and continue to monitor.
A woman at 41-weeks gestation is being induced. She is 2 cm dilated and is on oxytocin at 8 milliunits/minute. Based on the fetal heart rate tracing shown, the best initial response is to:
Continue to observe
Decrease the oxytocin
Place a fetal spiral electrode
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
The tracing shows tachysystole with emerging late decelerations and minimal variability:
5 contractions in 10 minutes
Deceleration nadirs occur after the peak of the contraction (late pattern)
Variability begins to trend toward minimal
The tracing has deteriorated while on oxytocin 8 mU/min, a common threshold for overstimulation
NCC and AWHONN emphasize that when tachysystole occurs with any fetal intolerance, the first action is to reduce or stop oxytocin.
Key NCC principles:
Late decelerations + tachysystole = uteroplacental insufficiency caused by excessive uterine activity
Interventions:
Stop or reduce oxytocin
Maternal repositioning
IV fluid bolus
Possible oxygen if other measures fail
Why the other options are incorrect:
A. Continue to observe — not acceptable with late decels + tachysystole.
C. Place a spiral electrode — this corrects signal quality, not uterine overstimulation or fetal oxygenation.
Thus, the best initial response is B. Decrease the oxytocin.
Amnioinfusion can cause what changes in the fetal heart rate tracing?
Improvement in fetal heart rate variability
Increase in fetal heart rate baseline
Resolution of variable decelerations
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NCC defines amnioinfusion as indicated for:
Recurrent variable decelerations caused by cord compression
Oligohydramnios reducing buffer around the cord
Expected effect:
Reduction or elimination of variable decelerations
Why the other answers are incorrect:
A. Variability does not improve with amnioinfusion.
B. Baseline FHR does not increase as a result of amnioinfusion.
Correct answer: C. Resolution of variable decelerations.
The most highly oxygenated blood in the fetal circulation is found in the
descending aorta
ductus venosus
pulmonary arteries
Comprehensive and Detailed Explanation From Exact Extract Sources:
In fetal physiology, the highest oxygen saturation exists in the umbilical vein, which then flows through the ductus venosus before entering the right atrium.
According to Creasy & Resnik Maternal-Fetal Medicine, and AWHONN physiologic foundations:
The umbilical vein carries oxygen-rich blood from the placenta (approx. 80% saturation).
Most of this blood bypasses the liver via the ductus venosus, which therefore contains the most highly oxygenated blood within the fetal circulatory system.
By contrast:
The descending aorta contains mixed blood with significantly lower oxygen content due to mixing after passage through the ductus arteriosus.
The pulmonary arteries in the fetus carry predominantly deoxygenated blood, since fetal lungs are fluid-filled and have high pulmonary vascular resistance.
Thus, the structure containing the highest fetal oxygen concentration is the ductus venosus.
When fetal arterial blood pressure increases, the baroreceptors send impulses to the vagus nerve resulting in:
Decreased heart rate
Decreased PO₂
Reflex tachycardia
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
Fetal baroreceptors, located primarily in the carotid sinus and aortic arch, respond to increases in fetal arterial pressure. When activated, they stimulate the vagus nerve, causing:
Reflex parasympathetic activation
Decreased FHR (vagal slowing)
This is a well-established physiologic mechanism referenced throughout NCC’s physiology domain. NCC emphasizes that variable decelerations, especially short deep drops, can occur when transient increases in fetal blood pressure from cord compression activate these baroreceptors.
Option B, decreased PO₂, relates to chemoreceptor-mediated responses—not baroreceptors.
Option C, reflex tachycardia, is mediated by sympathetic activation and occurs when BP falls, not rises.
Thus, the correct physiologic response is A. Decreased heart rate.
When the fetal heart rate is measured by a Doppler transducer and the intervals between heart beats are persistently identical, this shows as
absent variability
bradycardia
normal baseline
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources
Variability is created by beat-to-beat differences in fetal cardiac intervals due to autonomic nervous system modulation. AWHONN specifies that absent variability appears as “a near-straight line with minimal or no discernible oscillations,” which occurs when all beat intervals are identical.
Menihan notes that Doppler displays variability based on mechanical motion and will show flat, unchanging intervals when fetal autonomic modulation is suppressed, reflecting absent variability.
Bradycardia refers to a baseline <110 bpm and does not describe the uniformity of intervals. A normal baseline may still show variability; it cannot have identical beat-to-beat intervals, as this violates the definition of variability in NICHD terminology.
Simpson & Creehan state that absent variability is a significant marker of impaired fetal oxygenation or CNS depression.
An internal electronic fetal monitor tracing continues to record artifact despite equipment troubleshooting and replacement of the spiral electrode. The next action is to:
Auscultate the fetal heart rate
Provide oxygen
Reposition the woman
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
When internal monitoring continues to record artifact despite:
Changing the scalp electrode
Ensuring correct attachment
Checking cable connections
Confirming maternal movement is not the cause
NCC requires confirmation of fetal well-being using another modality.
The correct next step is direct auscultation with Doppler or fetoscope.
Why other answers are incorrect:
Oxygen is not indicated for equipment malfunction.
Repositioning does not resolve internal FHR artifact.
Thus, Auscultate the fetal heart rate is the appropriate next step.
A fetal heart rate tracing is abnormal. A change in maternal position and oxygen administration do not correct the pattern. Following birth, a fetal cord blood sample is taken:
pH = 7.25
PaCO₂ = 46 mm Hg
PaO₂ = 20 mm Hg
HCO₃ = 22 mEq/L
Base deficit = –4 mEq/L
These results are best interpreted as:
Acidosis
Hypoxia
Normal
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
Normal umbilical arterial values per NCC/AWHONN/Menihan:
pH: 7.20–7.30
PaCO₂: 45–55 mmHg
HCO₃: 20–24 mEq/L
Base deficit: 0 to –5 (normal to mild respiratory changes)
This sample shows:
pH 7.25 → normal
Base deficit –4 → no metabolic acidosis
HCO₃ normal
Slightly elevated PaCO₂, consistent with mild respiratory influence but still normal
PaO₂ 20 mmHg is normal for cord arterial blood
This profile is not acidotic (acidosis requires pH <7.10 and base deficit ≥12).
It also does not indicate hypoxia, which would present with metabolic acidosis.
Therefore: Normal.
A woman is admitted at 41-weeks gestation for fetal evaluation following a motor vehicle accident. She reports that she hit her abdomen on the steering wheel. The underlying physiology of the tracing is most likely:
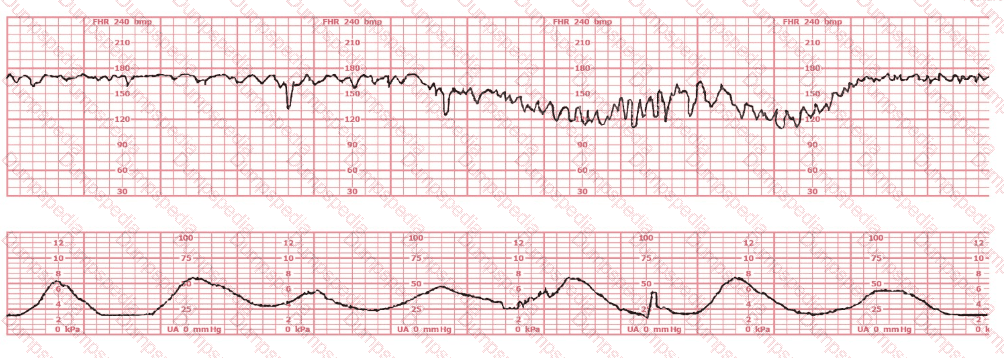
Cord accident
Fetal trauma
Placental abruption
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
This tracing shows recurrent late decelerations, decreased variability, and subtle baseline shifts—findings that strongly correspond to uteroplacental insufficiency. In trauma cases, NCC emphasizes that placental abruption is the most common fetal complication, caused by shearing forces separating the placenta from the uterine wall.
Key physiologic points per NCC/AWHONN/Menihan:
Maternal blunt abdominal trauma frequently leads to partial or concealed abruption.
Abruption produces decreased uteroplacental blood flow, resulting in:
Late decelerations
Minimal/absent variability
Baseline shifts or instability
Cord accident (option A) typically produces variable decelerations, not late-pattern decelerations.
Fetal trauma (option B) is extremely rare and does not produce a consistent deceleration pattern.
Thus, the physiology most consistent with this tracing and mechanism of injury is placental abruption.
The success of interventions to treat fetal hypoxia first depends on:
Improving maternal oxygenation
Minimizing uterine activity
Optimizing uteroplacental blood flow
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NCC/AWHONN emphasize that the primary goal of intrauterine resuscitation is to:
Optimize uteroplacental blood flow, which restores fetal oxygen delivery.
Key measures include:
Maternal repositioning (lateral)
Reducing tachysystole
IV fluid bolus
Correcting maternal hypotension
Stopping oxytocin
Treating underlying causes
Improving maternal oxygenation is supportive, but improving uteroplacental perfusion is the critical first determinant of resuscitation success.
Why the other answers are not first priority:
A. Oxygen — optional and no longer universally recommended unless maternal hypoxemia exists.
B. Minimizing uterine activity — essential, but still secondary to restoring perfusion.
Correct answer: C. Optimizing uteroplacental blood flow
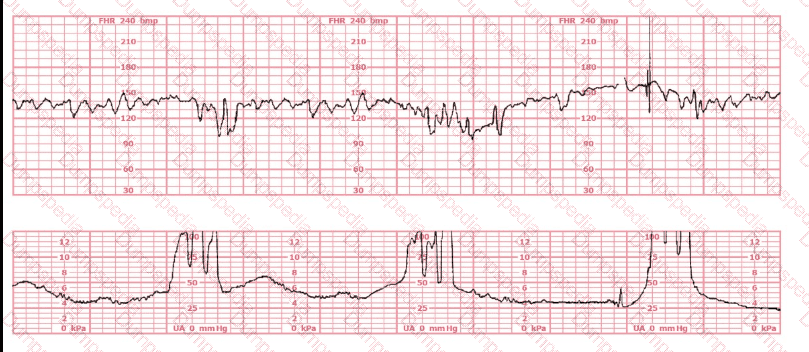
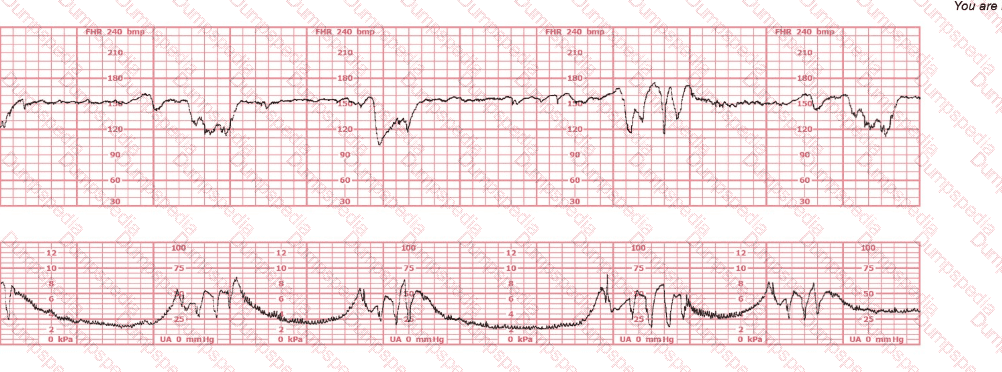
The decelerations seen in the fetal monitoring tracing shown are best described as:
Early
Late
Variable
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
Accurate classification of decelerations requires evaluating their shape, onset, nadir, recovery, relationship to contractions, and variability characteristics. NCC uses the NICHD standardized definitions, reinforced across AWHONN, Miller’s Pocket Guide, Menihan, Simpson, and Creasy & Resnik.
Key features in this tracing:
Abrupt onsetThe FHR drops rapidly from baseline to nadir in less than 30 seconds—this is the defining hallmark of a variable deceleration per NICHD.
Sharp V-shape and deep amplitudeThe tracing shows steep descents and ascents, characteristic of cord compression–type variable decelerations.
Inconsistent timing with contractionsThe decelerations do not begin at the start of contractions (as early decelerations would) and do not consistently begin after the peak of contractions (as late decelerations would). Variable decelerations can occur before, during, or after a contraction—exactly what is demonstrated here.
Rapid return to baselineAnother core feature of variable decelerations in NICHD/NCC definitions.
No uniform contraction relationshipEarly decelerations are symmetrical and mirror contractions. Late decelerations begin after the peak of the contraction. This strip does not match either pattern.
Differentiation per NCC-aligned definitions:
Early Decelerations:Gradual onset (>30 sec), nadir mirrors contraction peak, shallow, uniform.Not present.
Late Decelerations:Gradual descent, nadir after contraction peak, smooth shape.Not present.
Variable Decelerations:Abrupt onset (<30 sec), variable timing, sharp V-shape, rapid recovery, often with shoulders.Exactly matches the tracing.
Therefore, according to NICHD/NCC criteria, the decelerations shown are variable decelerations.
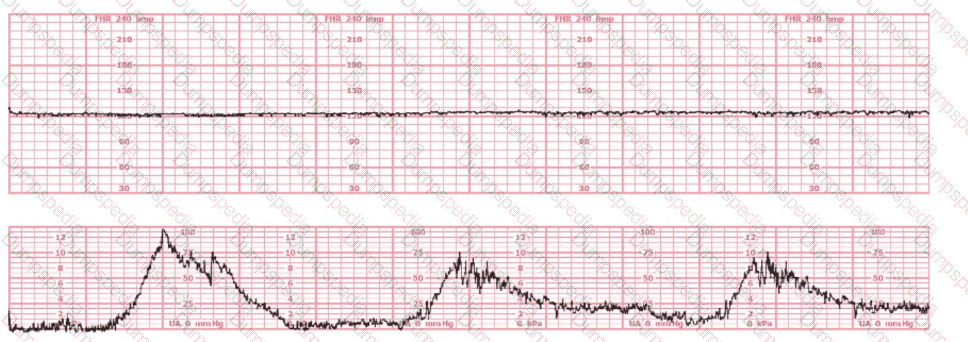
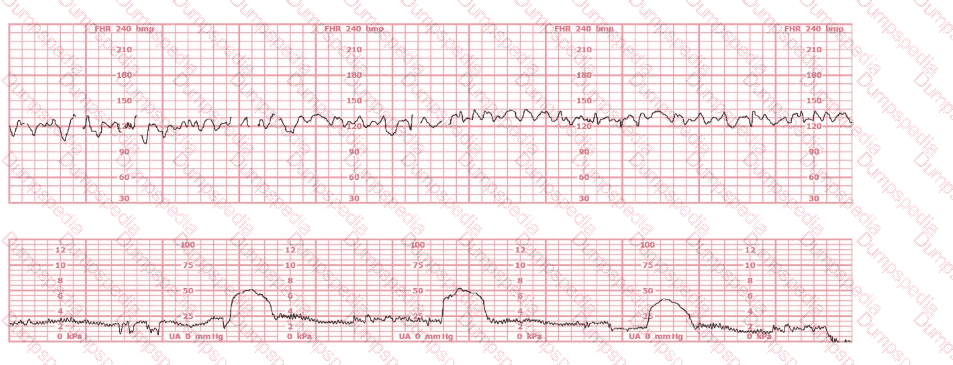
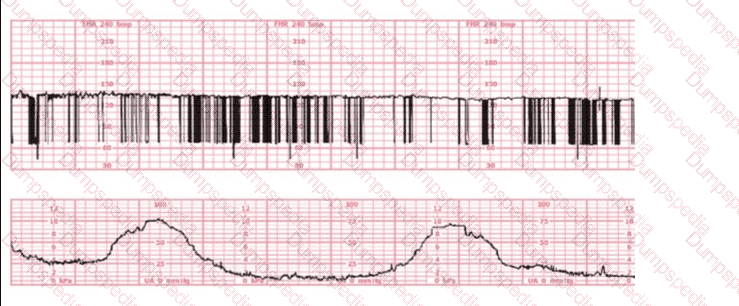
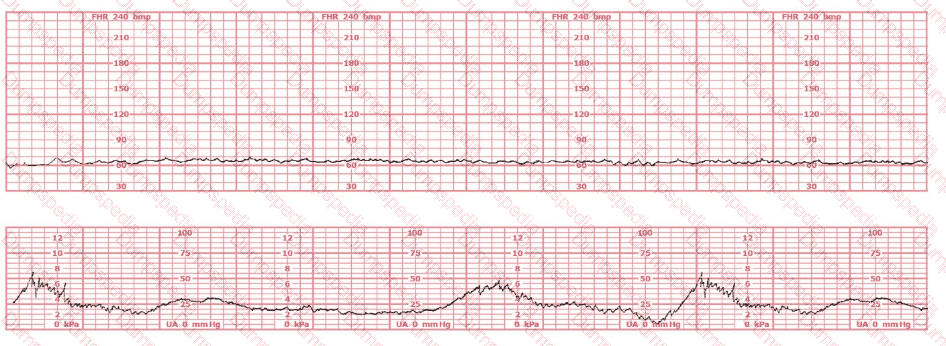
The most probable underlying fetal physiologic cause for this tracing would be:
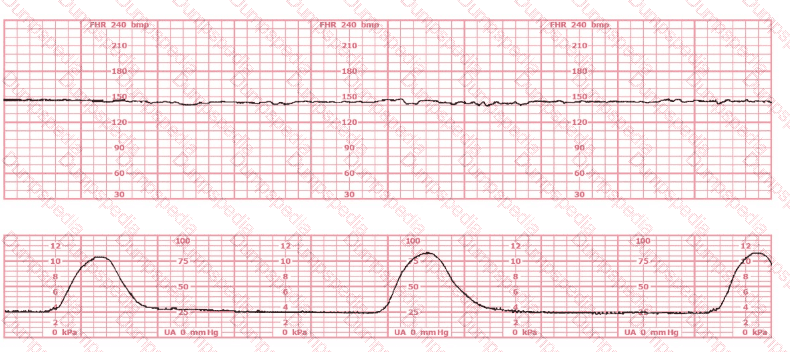
Myocardial hypoxic depression
Release of catecholamines
Vagal nerve stimulation in response to hypoxemia
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
This tracing shows:
Baseline ~145 bpm
Minimal variability
No accelerations or decelerations
Very little fluctuation → resembles a flat/minimal variability Category II tracing
The key physiologic mechanism behind minimal variability in the presence of a normal baseline and normal contraction pattern is most often:
Increased fetal sympathetic tone, driven by catecholamine release (epinephrine and norepinephrine).
NCC and AWHONN explain:
Catecholamine release (due to fetal stress, early hypoxemia, or maternal stress) results in:
Reduced beat-to-beat fluctuation
Minimal baseline variability
This is considered an early compensatory mechanism, not yet a decompensated hypoxic state.
Why the other answers are incorrect:
A. Myocardial hypoxic depression
Causes absent variability, NOT minimal variability.
Represents advanced or severe hypoxia. The FHR here is not absent variability.
C. Vagal stimulation in response to hypoxemia
Produces decelerations, especially late or prolonged.
This strip shows no decelerations, ruling this out.
Therefore the most accurate physiologic explanation is B. Release of catecholamines.
Based on the tracing shown, the first action should be to
administer vibroacoustic stimulation
assess maternal temperature
palpate for contractions
Comprehensive and Detailed Explanation From Exact Extract (No URLs or Links):
According to the NCC C-EFM exam outline and AWHONN Fetal Heart Monitoring Principles (2022), the first step when evaluating a concerning fetal heart rate pattern is to verify uterine activity, because the fetal response is often directly associated with contraction frequency, strength, or tachysystole. AWHONN states that “the clinician must confirm maternal–fetal physiology and uterine activity by palpation when interpreting any FHR pattern, as tocodynamometry may under- or overestimate uterine pressure.” Menihan’s Electronic Fetal Monitoring further emphasizes: “Always validate the contraction pattern via maternal abdominal palpation before proceeding with additional interventions.”
The tracing shows a late-appearing deceleration pattern with uncertain contraction correlation because the external toco waveform is inadequate (flat or poorly recorded). Before determining whether the decelerations are early, late, or variable, the clinician must confirm whether contractions are present, absent, or excessive. This step is listed as a core competency under Pattern Recognition & Intervention in the NCC Candidate Guide.
Therefore, palpating for contractions is the required first intervention.
This is a tracing of a multiparous woman in the second stage of labor. The vertex is at +3 station. This pattern has continued for the last 20 minutes. She has been pushing for 2½ hours, and oxytocin is infusing at 12 milliunits/minute. Management should include
increasing the oxytocin
preparing for cesarean birth
preparing for operative vaginal birth
Comprehensive and Detailed Explanation (From NCC C-EFM–Referenced Sources)
According to NCC C-EFM content guidance and AWHONN Fetal Heart Monitoring Principles (2022), recurrent variable and late patterns in second stage with descent to +2/+3 station require consideration of expediting delivery, especially when maternal effort is prolonged and oxytocin augmentation is already present.
Menihan & Simpson emphasize that with prolonged second stage, continued pushing beyond 2–3 hours, and vertex at +3 station, the evidence-based next step is operative vaginal birth, provided prerequisites are met. Cesarean is not indicated when the fetal head is already low and deliverable vaginally.
AWHONN and Creasy & Resnik state that increasing oxytocin when facing fetal stress and prolonged second stage is contraindicated, because tachysystole worsens fetal oxygenation and increases risk of fetal compromise.
Exact Extract Concepts Referenced:
– “Expedited delivery is recommended when recurrent decelerations persist in second stage and the head is low enough for operative vaginal birth.” (AWHONN Principles)
– “Oxytocin should be reduced or discontinued in the presence of nonreassuring patterns.” (Simpson, Obstetric Interventions)
– “Operative vaginal delivery is appropriate with full dilation, engaged head, and prolonged second stage.” (Menihan, Simpson; Creasy & Resnik)
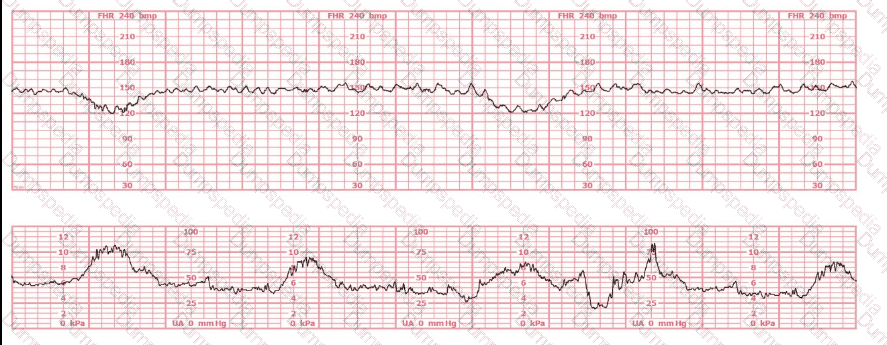
This tracing reflects
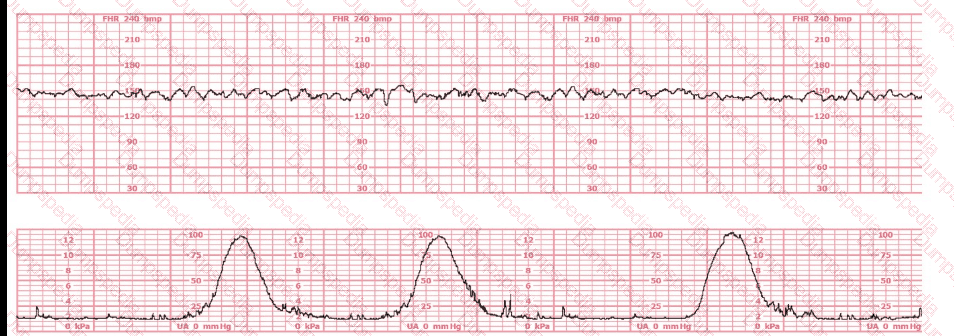
Minimal variability
Moderate variability
Sinusoidal pattern
Comprehensive and Detailed Explanation From Exact Extract (NCC-Recommended Sources Only)
The fetal heart rate (FHR) tracing shown demonstrates a baseline approximately 135–145 bpm with fluctuations of 6–25 bpm, a hallmark of moderate variability. Moderate variability is defined in all NCC-endorsed resources as the normal amplitude range of 6–25 bpm around the fetal baseline.
According to the AWHONN Fetal Heart Monitoring Principles & Practices (2022–2024), moderate variability is considered the single most reliable indicator of adequate fetal oxygenation and intact neurologic pathways, specifically reflecting well-functioning sympathetic and parasympathetic interplay.
The NICHD/NCC standardized definitions included in the NCC C-EFM Candidate Guide state:
Minimal variability: amplitude range ≤ 5 bpm
Moderate variability: amplitude range 6–25 bpm
Marked variability: amplitude > 25 bpm
Sinusoidal pattern: smooth, undulating waveform, 3–5 cycles per minute, equal amplitude, absent beat-to-beat variability
The tracing provided does not show the repetitive, smooth, wave-like pattern of a sinusoidal rhythm; nor does it show flattening associated with minimal variability. Instead, it includes continuous beat-to-beat fluctuation within the moderate range, without periods of absent or minimal variability.
Menihan’s Electronic Fetal Monitoring (5th ed.) and Simpson & Creehan’s Perinatal Nursing (5th ed.) both emphasize that moderate variability is:
A reassuring feature
Indicative of adequate fetal CNS oxygenation
Expected in a reactive, well-oxygenated fetus
A key criterion for Category I classification
Additionally, Miller’s EFM Pocket Guide reiterates that variability between 6–25 bpm is considered the normal (moderate) fetal autonomic response and is not a sinusoidal pattern, which has a fixed amplitude and frequency.
Therefore, based on NCC-standard definitions and the observed amplitude, the correct interpretation is moderate variability.
References (No URLs):
AWHONN Fetal Heart Monitoring Principles & Practices; NCC C-EFM Candidate Guide 2025; Simpson & Creehan Perinatal Nursing; Menihan Electronic Fetal Monitoring; Miller’s Pocket Guide to Fetal Monitoring; Creasy & Resnik Maternal-Fetal Medicine.
In the event of recurrent variable decelerations with thick meconium, amnioinfusion is recommended to:
Dilute thick meconium
Restore uterine blood flow
Treat oligohydramnios
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
Amnioinfusion is considered an intrauterine resuscitative intervention used specifically for recurrent variable decelerations caused by cord compression. NCC, AWHONN, Miller, and Menihan consistently teach that variables occur when the umbilical cord becomes compressed, reducing fetal oxygenation. When oligohydramnios or decreased amniotic fluid volume is present, the cord is more vulnerable to compression.
Why amnioinfusion is used:
Amnioinfusion works by:
Increasing intraamniotic fluid volume
Reducing umbilical cord compression
Decreasing the frequency and severity of variable decelerations
This directly targets the pathophysiology behind recurrent variables.
Why the other options are incorrect:
A. Dilute thick meconium – NOT supported by NCC
Historically, amnioinfusion was studied for meconium dilution, but major organizations—including NCC-aligned sources—state that amnioinfusion is NOT recommended for the sole purpose of diluting meconium. It does not reduce meconium aspiration syndrome and is no longer indicated for that purpose.
B. Restore uterine blood flow – NOT accurate
Uterine blood flow is addressed through maternal positioning, fluid bolus, reducing uterine tachysystole, and minimizing vasoconstriction—not via amnioinfusion. Amnioinfusion does not physiologically affect uterine perfusion.
C. Treat oligohydramnios – CORRECT
Recurrent variables with thick meconium often occur in the setting of low fluid, which worsens cord compression.
NCC-recommended indications include:
Recurrent variable decelerations unresponsive to repositioning
Suspected or confirmed oligohydramnios
Thick meconium may be associated with low fluid, but the purpose of amnioinfusion is to alleviate cord compression by restoring fluid volume, not to dilute the meconium.
Thus, the correct answer is C. Treat oligohydramnios.
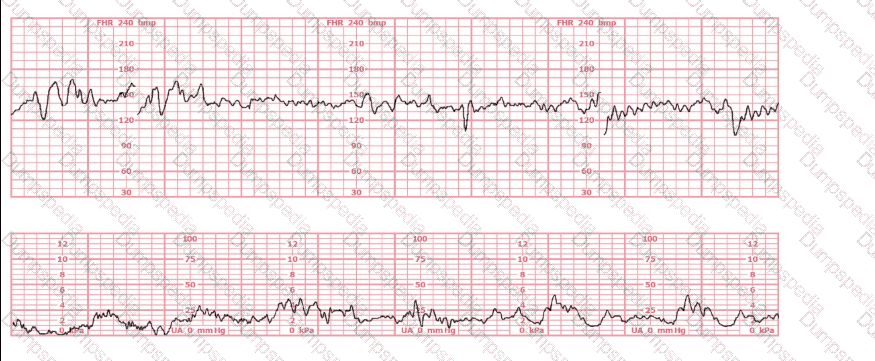
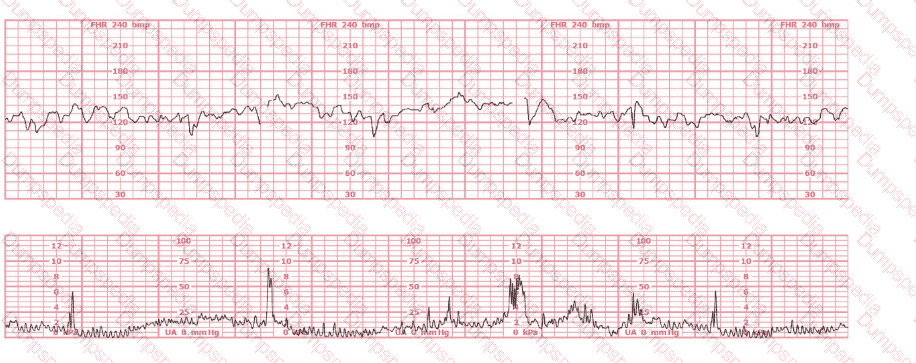
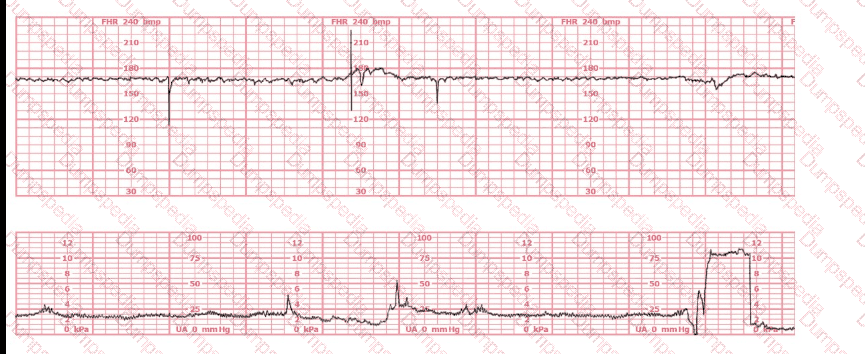
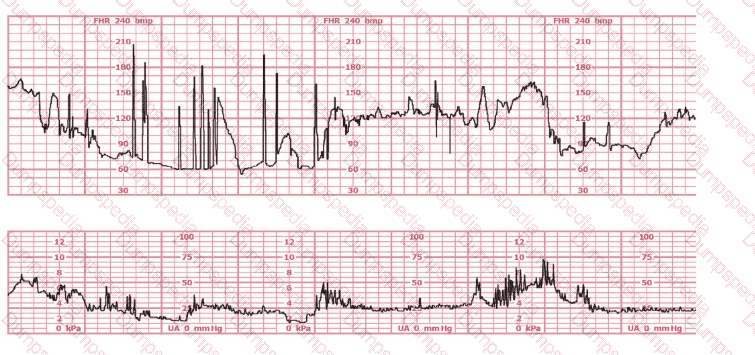
This fetal heart rate tracing is obtained upon the woman's admission to labor and delivery. This tracing is most reflective of:
Atrial flutter
Complete heart block
Fetal dysrhythmia
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
When evaluating an admission tracing, NCC emphasizes determining whether the pattern represents baseline variability abnormalities, signal artifact, or an underlying fetal cardiac rhythm disturbance. The strip shown contains clear features of a fetal dysrhythmia, which NCC and AWHONN describe as an irregular rhythm characterized by inconsistent R–R intervals or intermittent missed beats.
Key features in this tracing:
Extremely irregular FHR signalThe pattern shows abrupt vertical spikes, inconsistent spacing, and intermittent loss of coherent waveform. NCC teaches that this appearance is typical of irregular ventricular conduction or premature atrial/ventricular contractions.
Wide variability in beat spacingBeat intervals vary significantly, suggesting ectopic beats or conduction abnormalities rather than a stable rhythm such as heart block or atrial flutter.
Sensor not malfunctioningThe lower uterine activity channel is smooth and consistent, meaning the upper channel’s abrupt changes represent true FHR signal irregularity, not artifact.
Why the incorrect answers are ruled out:
A. Atrial flutter – NOT supported
Atrial flutter produces a very fast, regular atrial rate (typically 300 bpm) with a repetitive saw-tooth pattern.
It does not produce the highly irregular beat-to-beat pattern seen here.
FHR in atrial flutter appears more organized, not chaotic.
B. Complete heart block – NOT supported
Complete heart block (third-degree AV block) produces a very slow, regular ventricular rate, commonly 50–70 bpm, with a dissociation between atrial and ventricular rhythms.
The tracing here does not show a slow, steady baseline.
Instead, the rhythm is highly irregular with spikes and losses—not characteristic of AV block.
C. Fetal dysrhythmia – CORRECT
NCC, AWHONN, Miller, and Menihan describe fetal dysrhythmias as:“Irregular, inconsistent FHR patterns due to premature atrial contractions (PACs), premature ventricular contractions (PVCs), or intermittent conduction disturbances.”
The hallmark is an irregular rhythm, often appearing as abrupt spikes or missing beats on the monitor.
The tracing shown matches these characteristics precisely.
Therefore, the tracing is most consistent with fetal dysrhythmia, typically benign PACs/PVCs, and is the correct answer.
A woman at 39-weeks gestation is being induced. She has chronic hypertension controlled by methyldopa (Aldomet). Spontaneous rupture of membranes has occurred; she is 10 cm dilated and at +1 station. The fetal monitor tracing shown is obtained by spiral electrode and tocodynamometer. The next best appropriate action is to:
Administer terbutaline
Consider amnioinfusion
Modify pushing
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
The tracing shows recurrent variable decelerations deepening during contractions as the patient is fully dilated and at +1 station.
NCC’s Pattern Recognition and Intervention framework states:
During second stage (complete dilation), variable decelerations commonly occur from cord compression caused by head descent and maternal pushing efforts.
The FIRST correction for pushing-associated recurrent variable decelerations is modifying the pushing technique:
Side-lying pushing
Pushing with every other contraction
Open-glottis pushing
Allowing passive descent
These measures relieve head compression and reduce the severity of variable decelerations.
Why the other answers are incorrect
A. Administer terbutaline
Terbutaline is given for tachysystole with fetal intolerance.
This tracing does not show tachysystole.
The pattern is timing-related to pushing, not uterine overstimulation.
B. Consider amnioinfusion
Amnioinfusion is used for recurrent variable decelerations before complete dilation, when membrane rupture + low fluid is suspected.
At 10 cm and +1, the fetal head is deep in the pelvis, and the cause of variables is head compression, not cord compression due to oligohydramnios.
Also, amnioinfusion is impractical and not beneficial at this stage.
Therefore, the correct answer is C. Modify pushing.
(Full question statement)
The fetal heart rate tracing shown is obtained upon the woman's admission to labor and delivery. This tracing is most consistent with what maternal condition?
Eisenmenger's syndrome
Sickle cell anemia
Systemic lupus erythematosus
Comprehensive and Detailed Explanation From Exact Extract (NCC C-EFM sources: AWHONN, Miller’s Pocket Guide, Menihan, Simpson, Creasy & Resnik, 2025 Candidate Guide)
The tracing displays baseline fetal bradycardia, with a rate near 100 bpm, minimal variability, and preserved periodic response. According to AWHONN’s Fetal Heart Monitoring Principles & Practices and Menihan’s Electronic Fetal Monitoring, maternal conditions that reduce oxygen-carrying capacity—including maternal anemia—can lead to lower fetal oxygen delivery, prompting a fetal compensatory bradycardic baseline.
Creasy & Resnik’s Maternal-Fetal Medicine notes that sickle cell anemia decreases maternal hemoglobin function even when maternal vital signs appear stable, reducing uteroplacental oxygen transport. Fetuses of mothers with sickling disorders may demonstrate lower resting fetal heart rates due to chronic mild hypoxemia.
Conversely, Eisenmenger’s syndrome is associated with severe maternal cyanosis and high fetal mortality, often producing late decelerations and growth restriction rather than mild bradycardia. Systemic lupus erythematosus (SLE) is commonly associated with heart block (especially with anti-Ro/SSA antibodies), which is not displayed here, as true heart block presents with a fixed atrial–ventricular dissociation and FHR < 60 bpm.
Thus, based on fetal physiology and maternal disease correlations taught in NCC-recommended sources, the tracing is most consistent with maternal sickle cell anemia.
When R-R intervals are short, the fetal heart rate is
fast
normal
slow
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources
The fetal heart rate is calculated from the interval between consecutive R waves in the fetal ECG. Shorter R-R intervals indicate more beats per unit of time, therefore resulting in a higher heart rate. AWHONN and Menihan both note that fetal ECG monitoring measures instantaneous rate based on R-R spacing, and “shorter intervals correspond to fetal tachycardia.”
Simpson & Creehan reinforce that fetal heart rate variability and baseline are derived from these R-R intervals, with shorter intervals consistently producing faster rates. Miller’s Pocket Guide describes the relationship simply: “Short R-R = faster rate; long R-R = slower rate.”
The duration of a contraction is best represented by which colored arrow?
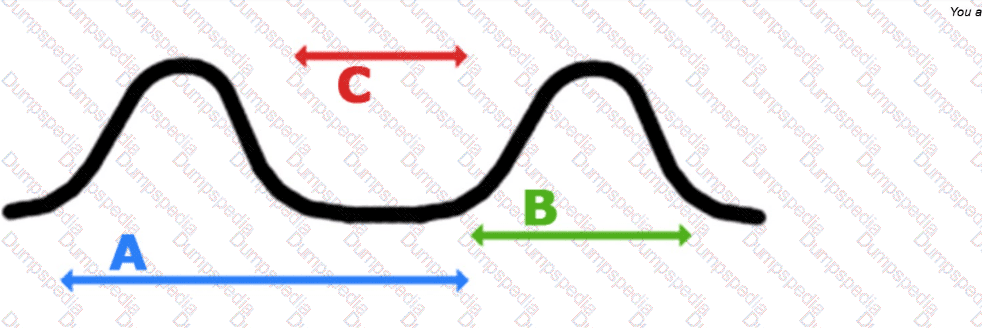
Blue (A)
Green (B)
Red (C)
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
Contraction duration is defined as the length of time from the beginning of a contraction to the end of the same contraction (NICHD uterine activity definitions).
In the diagram:
Green arrow (B) spans one individual contraction from rise → peak → return to baseline.
Blue arrow (A) measures the interval between contractions (frequency).
Red arrow (C) measures peak-to-peak amplitude shape, not duration.
Therefore, the green arrow correctly identifies contraction duration.
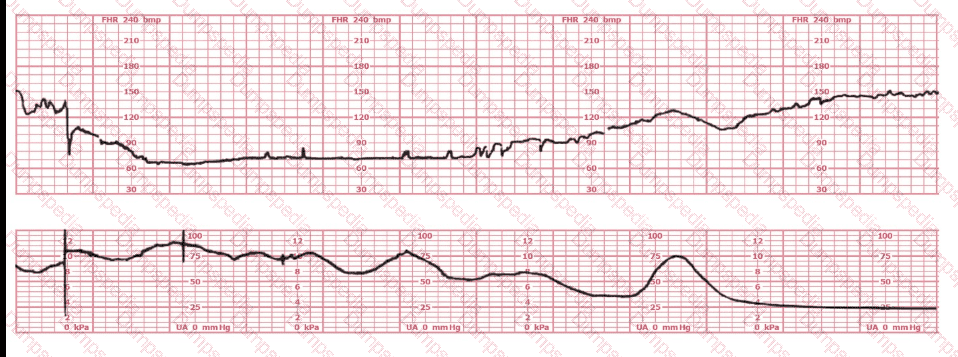
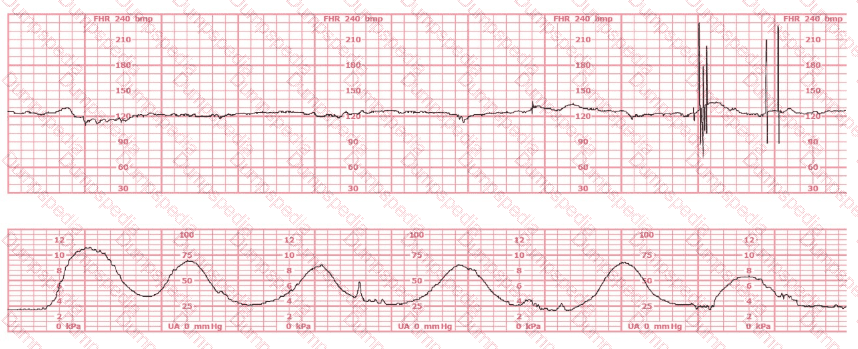
This tracing demonstrates:
Bradycardia
Category III tracing
Prolonged deceleration
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
A prolonged deceleration is defined by NICHD and NCC as:
A deceleration lasting ≥2 minutes but <10 minutes
Decrease in FHR of ≥15 bpm
Can occur with or without uterine contractions
This tracing shows:
A deep drop in FHR down to ~60–70 bpm
Duration lasting several minutes
Recovery back to baseline
Moderate variability present afterward
Because variability remains present and the tracing does not show:
Absent variability
Recurrent late decelerations
Recurrent variable decelerations with absent variability
Bradycardia for ≥10 minutes
…it does not meet criteria for Category III.
It is also not bradycardia, because bradycardia requires:
Baseline <110 bpm for 10 minutes or longer
Therefore the correct interpretation is a prolonged deceleration.
The factor that differentiates a prolonged deceleration from bradycardia is:
Baseline rate
Length of time it lasts
Relationship to contractions
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
NICHD/NCC definitions:
Prolonged deceleration: decrease in FHR ≥15 bpm lasting 2 to 10 minutes
Bradycardia: baseline FHR <110 bpm lasting ≥10 minutes
The differentiating factor is duration, not rate and not contraction relationship.
Before 10 minutes → prolonged deceleration
At or beyond 10 minutes → new baseline → bradycardia
Thus, the factor that differentiates the two is length of time it lasts.
A reliable indicator of fetal oxygenation is fetal
heart rate accelerations
movement
regular sleep–wake cycles
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources
AWHONN and NICHD definitions state that fetal accelerations are a strong indicator of adequate fetal oxygenation and neurologic integrity. Accelerations reflect intact sympathetic and parasympathetic balance and adequate oxygen reserve.
Simpson & Creehan emphasize accelerations as “the most reliable sign of fetal well-being,” because they require intact autonomic function, sufficient pH, and adequate oxygenation. Menihan also identifies accelerations as the most reassuring feature on a fetal heart tracing.
Fetal movement is helpful but not directly reflective of oxygenation, as movements can decline for non-hypoxic reasons (sleep cycles, maternal sedation). Regular sleep–wake cycles are normal developmental neurologic patterns and not oxygenation markers.
Creasy & Resnik reinforce that “presence of accelerations reliably indicates absence of metabolic acidemia.”
The main reason intrauterine pressure catheters are placed is to:
Define the quality of the fetal baseline
Determine the contraction pattern
Rule out artifact
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
Intrauterine pressure catheters (IUPCs) are an internal uterine activity monitoring device used when external tocodynamometry does not provide adequate assessment of contraction strength or frequency. According to NCC, AWHONN, Miller, and Menihan, the primary indication for placing an IUPC is to obtain accurate, quantitative measurement of uterine activity.
Purpose of IUPC (per NCC and AWHONN):
Measures exact intrauterine pressure in mmHg
Calculates Montevideo units (MVUs) to evaluate adequacy of labor
Clearly differentiates:
Frequency
Duration
Strength (intensity)
Resting tone
NCC explicitly lists the primary purpose as:
“Accurate assessment of uterine contraction pattern and intensity.”
Why the other options are incorrect:
A. Define the quality of the fetal baseline – Incorrect
Fetal heart rate (FHR) baseline quality is determined by fetal ECG or FSE, not IUPC.
IUPCs monitor the uterus, not the fetal cardiac signal.
C. Rule out artifact – Incorrect
While an IUPC can reduce artifact from the toco, this is not its primary purpose.
Artifact is more commonly an issue with external FHR monitoring, corrected by repositioning or placing a fetal scalp electrode—not by using an IUPC.
Correct Answer:
B. Determine the contraction pattern
This aligns directly with NCC’s Electronic Monitoring Equipment domain: IUPCs provide the most accurate and reliable measurement of uterine activity when external monitoring is inadequate.
Tachysystole can have a negative effect on fetal oxygenation during labor by
blocking active transport of oxygen to the fetus
increasing maternal blood pressure
interfering with reperfusion of the intervillous space
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources
NCC-recommended physiology references (AWHONN, Simpson & Creehan, Menihan, Creasy & Resnik) consistently state that the primary mechanism by which tachysystole affects fetal oxygenation is reduced uteroplacental perfusion, specifically through impaired intervillous space reperfusion.
During a normal contraction cycle, the fetus receives oxygen between contractions, when the uterus relaxes and maternal blood re-enters the intervillous space. AWHONN’s Fetal Heart Monitoring Principles & Practices explains that tachysystole—defined as more than five contractions in 10 minutes averaged over 30 minutes—shortens or eliminates the relaxation phase, preventing adequate placental reoxygenation.
Simpson & Creehan highlight that “tachysystole decreases uteroplacental blood flow and interferes with replenishment of oxygenated maternal blood in the intervillous space.” Menihan emphasizes that fetal hypoxemia in tachysystole results from interrupted perfusion, not from altered oxygen transport or maternal hemodynamic changes. Creasy & Resnik confirm that uterine overactivity reduces intervillous perfusion during contractions and impairs fetal oxygen exchange.
Thus, the physiologic problem is failure of the intervillous space to reperfuse, which compromises fetal oxygenation.


TESTED 14 Jul 2026